Screening
Identifying depleted patients or patients with a high risk of nutritional depletion, can both be a task of the doctor, the nursing team and/ or the dietician. A structured screening of patients at admission and during hospitalization could improve a rapid identification of risk patients.
Screening tools
There are several validated screening tools used in the Netherlands, such as the SNAQ, MUST and NRS 2002.The SNAQ
The SNAQ (Short Nutritional Assessment Questionaire): developed by the VU university medical centre in Amsterdam in 2003.
The MUST
The MUST (Malnutrition Universal Screening Tool) was developed in England and is used by dieticians of the Maastricht UMC+.
The NRS 2002
The NRS 2002 (Nutritional Risk Screening 2002) is recommended to hospitals by the ESPEN (European Society of Enteral and Parenteral Nutrition) organisation.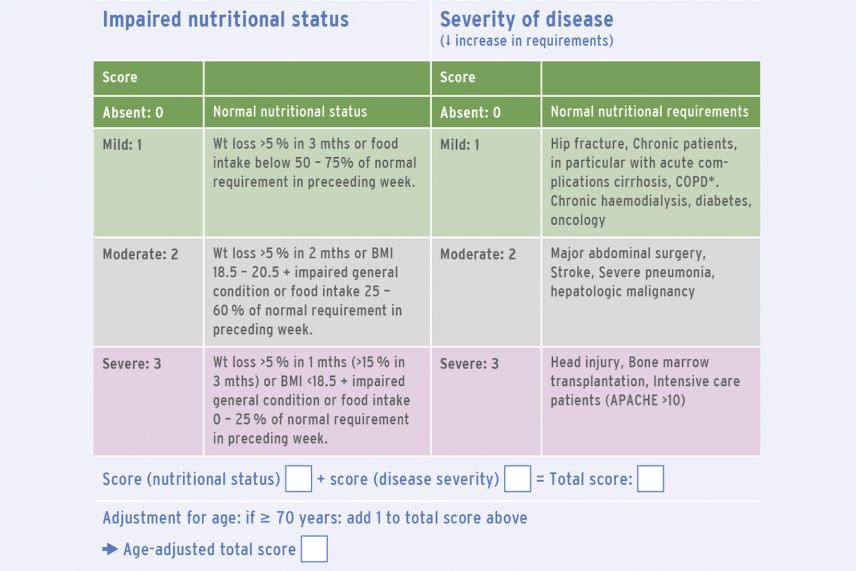
Collected data
Most screening tools collect the following data:- Percentage of weight loss: 5% within one month or 10% within six months;
- Factors that disturb food intake (such as less appetite, diminished taste, aversion or nausea, dry or painful mouth, problem with swallowing or passage and other problems);
- BMI<20
- Need for information
See the website of Fight Malnutrition and the E.S.P.E.N. Clinical Guidelines. Nutrition Screening, Assessment, and Intervention in Adults (2011) for more information on this subject.
Clinical signs of malnutrition
A doctor can use 'clinical signs' to discover malnutrition on the ward. It can give valuable information, although experience is needed. It is a subjective judgement. Underweight can be camouflaged with oedema or ascites. A set of points regarding the ‘clinical signs’:- appearance of the patient (hollow face)
- reaction (apathetic, tired)
- handshake (weak)
- condition of the skin (dry, pale, eventually bruises)
- condition of the hair (dull)
- strength of breathing muscles: tested by blowing a paper(weak)
- a sick impression
- no interest for environment
- diminished approachability